
What are prostatic calculi (prostate stones)? Do they affect sexual function?
What are prostatic calculi (prostate stones)? Do they affect sexual function?











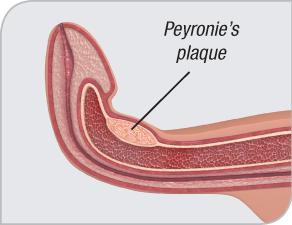
Peyronie’s disease is a disorder that causes areas of hardened scar tissue called plaques to form on the penis, just under the surface of the skin. These plaques make the penis less flexible. As a result, men with Peyronie’s disease have a noticeable curve in their penis. The penis may shorten as well.
Sexual intercourse can be difficult for men with Peyronie’s disease, especially if their curve is severe. Men may also experience pain and have problems with erections.
Experts aren’t sure what, exactly, causes Peyronie’s disease. It is believed to be a wound healing disorder. A man may injure his erect penis, such as through vigorous sex, and not even be aware that he has done so. However, the injury does not heal as it should. Instead, an excessive amount of scar tissue develops and does not break down as it typically would.
It’s also possible that some cases of Peyronie’s disease are inherited.
Peyronie’s disease occurs in two stages. The first is the “active” phase, which occurs during the first twelve to twenty-four months. During this phase, the disease progresses and the penis continues to bend.
Eventually, Peyronie’s disease stabilizes. This is called the “chronic” phase. At this time, pain usually subsides and the curve usually doesn’t worsen.
Not all men with Peyronie’s disease require treatment. For some, the condition goes away on its own. For others, the condition is not severe enough to require treatment.
However, many men decide to have treatment, which may involve surgery. Nonsurgical treatments are also available.
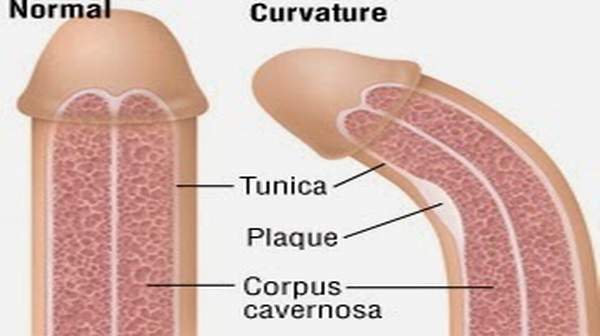
Plaques form on the tunica albuginea, the flexible tissue that surrounds other tissue that fills with blood during an erection. Because the plaques are hardened scar tissue, they cause the tunica albuginea to lose its elastic quality. This makes the penis bend when erect.
Usually, the plaques are found on the upper side of the penis, but they can be found on the underside, too. Sometimes they look like small dents; other times, they form all around the penis, giving it an hourglass look.
Surgery is the most common method. Tunica albuginea plication involves stitching tissue on the opposite side of the affected area to even out the bend. More severe cases are treated with a plaque incision and grafting procedure. Surgeons cut into the plaque and fill it with human or animal tissue.
Peyronie’s disease is a condition that causes hardened plaques to form just under the skin of the penis. As a result, the penis loses flexibility and develops a distinct curve, sometimes to the point that sexual intercourse is difficult or impossible.
Men with Peyronie’s disease often feel pain and experience erectile dysfunction. But the condition can take an emotional and psychological toll as well. Men may feel depressed that their intimate relationships have changed, frustrated that they can’t perform like they used to, and anxious about satisfying their partner.
Peyronie’s disease can, in fact, have an impact on partners. In 2016, the Journal of Sexual Medicine published a study by Canadian researchers that shed some light on Peyronie’s effects on female partners.
Couples facing Peyronie’s disease are encouraged to keep the lines of communication open, especially in sexual matters. They might need to make some adjustments to their sexual routine, but it’s still possible to be intimate. Some couples in this situation benefit from sex therapy, which can help them express and work through their sexual concerns, needs, and relationship issues.
Peyronie’s disease is characterized by areas of bone-like collagen plaques that form inside the penis. Because these plaques are hard and inflexible, they cause the penis to bend. Peyronie’s disease can be painful and make sexual intercourse difficult.
The exact cause of Peyronie’s disease is unknown, but it is believed to be a wound healing disorder. In other words, the penis is injured and doesn’t heal properly. Peyronie’s disease may also be genetic or linked to certain connective tissue disorders like Dupuytren's contracture.
Personal health risk factors may also be involved. For example, high blood sugar and tobacco use may make it harder for wounds to heal normally. These factors could, indirectly, make a man more likely to develop Peyronie’s disease. Other potential risk factors include diabetes, heart disease, alcohol use, and high cholesterol.
In 2015, a team of Italian scientists investigated erectile dysfunction (ED), smoking, diabetes, and high blood pressure as possible risk factors for Peyronie’s disease. After collecting data from a group of 279 men (97 with Peyronie’s disease, 182 without), they found that cigarette smoking, high blood pressure, and ED were associated with Peyronie’s disease, but diabetes was not.
These results do not mean that any of these conditions cause Peyronie’s disease. The scientists explained that more study is necessary to see if removing a potential risk factor reduces rates of Peyronie’s disease.
Scientists aren’t sure exactly some men with Peyronie’s disease also have ED, but the following factors might be involved:
If a man has ED along with Peyronie’s disease, he should talk to his doctor. The two conditions can be managed and a doctor can help determine what course of treatment is most appropriate.
One of the hallmarks of Peyronie’s disease is curvature of the penis. Plaques – areas of hardened scar tissue – cause the penis to lose some of its elasticity. This can make it bend when erect. For some men, the degree of curvature is so severe that they cannot have sex at all.
In July 2014, the International Journal of Impotence Research published a study that examined whether the degree and direction of a man’s curvature was associated with erectile dysfunction. They focused on vasculogenic ED, which involves poor blood flow to the penis.
The researchers found that the extent and direction of curvature did not appear to be related to ED.
“The role of [Peyronie’s disease] in the development of ED remains unclear at the present time,” they said.
Surgical treatment for Peyronie’s disease is usually considered when a man is in the stable phase. At this point, the curvature has reached a plateau – not worsening, but not getting better.
Physicians will also consider the type of curvature and degree of erectile function when making decisions about surgery.
The most common surgical treatments for Peyronie’s disease include the following:
Nesbit Procedure (Tunica Albuginea Plication). The tunica albuginea is a thin layer of tissue that envelops the corpora cavernosa – two chambers of spongy tissue that fill with blood during an erection. Plaques caused by Peyronie’s disease form in the tunica albuginea.
During this procedure, the surgeon straightens the penis by folding small portions of the tunica albuginea on the opposite side of the curve. (Sometimes, these small portions are removed.) The surgeon then stitches the area, keeping the penis straight.
Depending on the type of surgery and the man’s anatomy, there might be some penile shortening or loss of penile sensitivity after these procedures.
For men who have the Nesbit procedure or plaque incision and grafting, problems with erections could develop.
Concerned patients should ask their doctors about these issues. Resulting erectile dysfunction (ED) is usually treatable.
Men who are in the “active” stage of Peyronie’s disease, when the condition is still progressing, may choose nonsurgical treatments. Such treatments could include the following:
In some cases, medication is injected directly into the plaques themselves. Verapamil and interferon are two such substances, which are hypothesized to stop the development of collagen, the protein from which the plaques are made. They are also suggested to help “remodel” the scar tissue, making the plaques smaller as the area heals. However, there are conflicting reports regarding the efficacy of these therapies in the treatment of Peyronie’s disease.
This technique involves wearing a special device designed to straighten the penis. This device pulls the penis straight. Wearing the traction device between six and nine hours a day (with thirty minute breaks every two hours) appears to have the best results, according to recent research. Traction therapy may also help restore some lost penile length. Apparently, more research is required to elucidate whether this therapy is a viable option for patients with Peyronie’s disease.
VEDs are sometimes used by men with erectile dysfunction (ED). But there are some studies demonstrating that it might also help men with Peyronie’s disease. To use a VED, a man places a clear plastic cylinder over his penis. The cylinder is connected to a pump, which, when activated, creates a vacuum. Once an erection has formed, a constriction ring is placed at the base to keep it strong for whatever duration is needed.



