Medical causes
Problems with male fertility can be caused by a number of health issues and medical treatments. Some of these include:
- A varicocele is a swelling of the veins that drain the testicle. It's the most common reversible cause of male infertility. Although the exact reason that varicoceles cause infertility is unknown, it may be related to abnormal testicular temperature regulation. Varicoceles result in reduced quality of the sperm.
Treating the varicocele can improve sperm numbers and function, and may potentially improve outcomes when using assisted reproductive techniques such as in vitro fertilization.
- Some infections can interfere with sperm production or sperm health or can cause scarring that blocks the passage of sperm. These include inflammation of the epididymis (epididymitis) or testicles (orchitis) and some sexually transmitted infections, including gonorrhea or HIV. Although some infections can result in permanent testicular damage, most often sperm can still be retrieved.
- Ejaculation issues.Retrograde ejaculation occurs when semen enters the bladder during orgasm instead of emerging out the tip of the penis. Various health conditions can cause retrograde ejaculation, including diabetes, spinal injuries, medications, and surgery of the bladder, prostate or urethra.
Some men with spinal cord injuries or certain diseases can't ejaculate semen, even though they still produce sperm. Often in these cases sperm can still be retrieved for use in assisted reproductive techniques.
- Antibodies that attack sperm.Anti-sperm antibodies are immune system cells that mistakenly identify sperm as harmful invaders and attempt to eliminate them.
- Cancers and nonmalignant tumors can affect the male reproductive organs directly, through the glands that release hormones related to reproduction, such as the pituitary gland, or through unknown causes. In some cases, surgery, radiation or chemotherapy to treat tumors can affect male fertility.
- Undescended testicles.In some males, during fetal development one or both testicles fail to descend from the abdomen into the sac that normally contains the testicles (scrotum). Decreased fertility is more likely in men who have had this condition.
- Hormone imbalances.Infertility can result from disorders of the testicles themselves or an abnormality affecting other hormonal systems including the hypothalamus, pituitary, thyroid and adrenal glands. Low testosterone (male hypogonadism) and other hormonal problems have a number of possible underlying causes.
- Defects of tubules that transport sperm.Many different tubes carry sperm. They can be blocked due to various causes, including inadvertent injury from surgery, prior infections, trauma or abnormal development, such as with cystic fibrosis or similar inherited conditions.
Blockage can occur at any level, including within the testicle, in the tubes that drain the testicle, in the epididymis, in the vas deferens, near the ejaculatory ducts or in the urethra.
- Chromosome defects.Inherited disorders such as Klinefelter's syndrome — in which a male is born with two X chromosomes and one Y chromosome (instead of one X and one Y) — cause abnormal development of the male reproductive organs. Other genetic syndromes associated with infertility include cystic fibrosis, Kallmann's syndrome and Kartagener's syndrome.
- Problems with sexual intercourse.These can include trouble keeping or maintaining an erection sufficient for sex (erectile dysfunction), premature ejaculation, painful intercourse, anatomical abnormalities such as having a urethral opening beneath the penis (hypospadias), or psychological or relationship problems that interfere with sex.
- Celiac disease.A digestive disorder caused by sensitivity to gluten, celiac disease can cause male infertility. Fertility may improve after adopting a gluten-free diet.
- Certain medications.Testosterone replacement therapy, long-term anabolic steroid use, cancer medications (chemotherapy), certain antifungal medications, some ulcer drugs and certain other medications can impair sperm production and decrease male fertility.
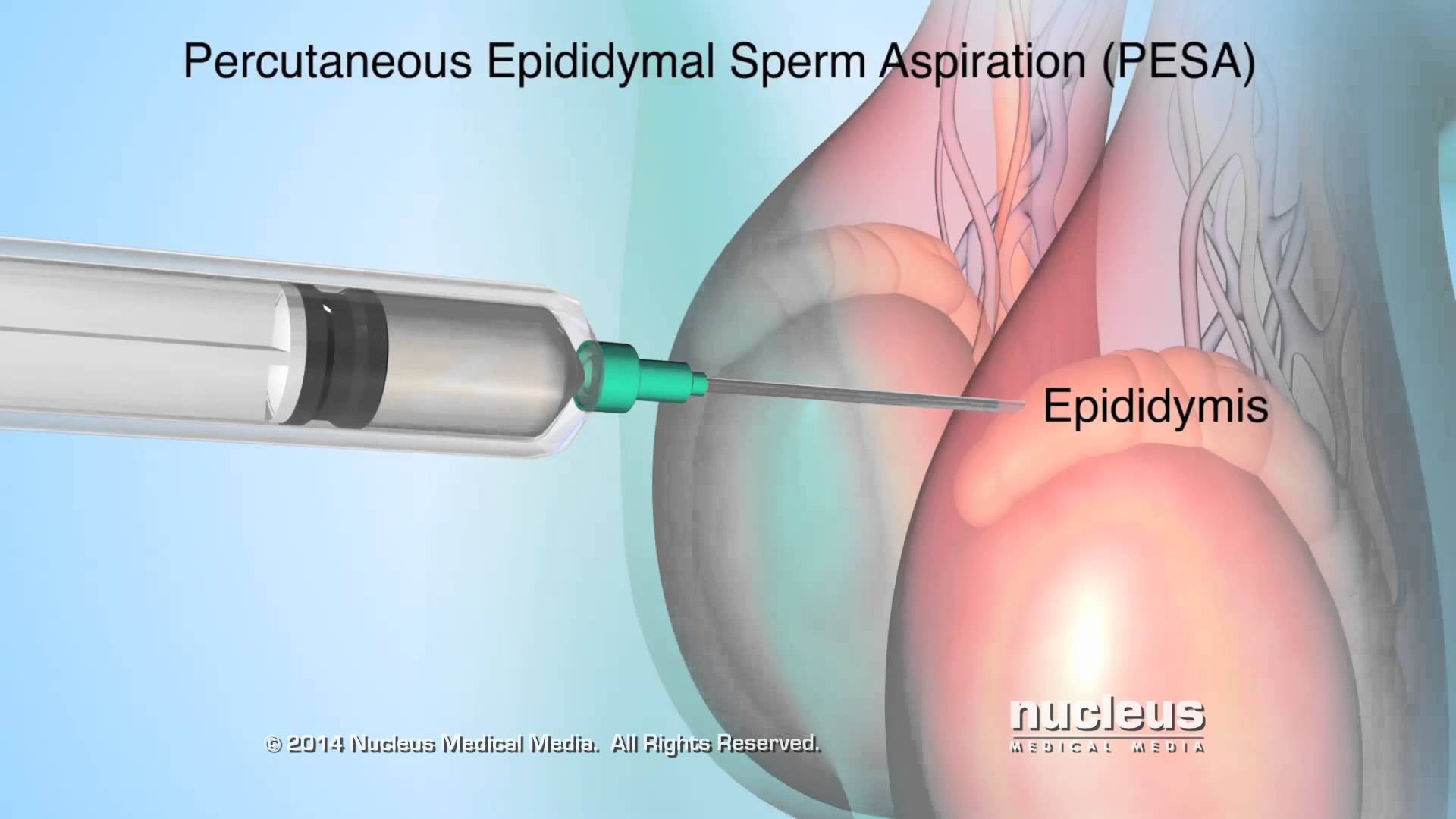
- Prior surgeries.Certain surgeries may prevent you from having sperm in your ejaculate, including vasectomy, inguinal hernia repairs, scrotal or testicular surgeries, prostate surgeries, and large abdominal surgeries performed for testicular and rectal cancers, among others. In most cases, surgery can be performed to either reverse these blockage or to retrieve sperm directly from the epididymis and testicles.
Environmental causes
Overexposure to certain environmental elements such as heat, toxins and chemicals can reduce sperm production or sperm function. Specific causes include:
- Industrial chemicals.Extended exposure to benzenes, toluene, xylene, pesticides, herbicides, organic solvents, painting materials and lead may contribute to low sperm counts.
- Heavy metal exposure.Exposure to lead or other heavy metals also may cause infertility.
- Radiation or X-rays.Exposure to radiation can reduce sperm production, though it will often eventually return to normal. With high doses of radiation, sperm production can be permanently reduced.
- Overheating the testicles.Elevated temperatures impair sperm production and function. Although studies are limited and are inconclusive, frequent use of saunas or hot tubs may temporarily impair your sperm count.
Sitting for long periods, wearing tight clothing or working on a laptop computer for long stretches of time also may increase the temperature in your scrotum and may slightly reduce sperm production.
Health, lifestyle and other causes
Some other causes of male infertility include:
- Illicit drug use.Anabolic steroids taken to stimulate muscle strength and growth can cause the testicles to shrink and sperm production to decrease. Use of cocaine or marijuana may temporarily reduce the number and quality of your sperm as well.
- Alcohol use.Drinking alcohol can lower testosterone levels, cause erectile dysfunction and decrease sperm production. Liver disease caused by excessive drinking also may lead to fertility problems.
- Tobacco smoking.Men who smoke may have a lower sperm count than do those who don't smoke. Secondhand smoke also may affect male fertility.
- Emotional stress.Stress can interfere with certain hormones needed to produce sperm. Severe or prolonged emotional stress, including problems with fertility, can affect your sperm count.
- Obesity can impair fertility in several ways, including directly impacting sperm themselves as well as by causing hormone changes that reduce male fertility.
Certain occupations including welding or those involving prolonged sitting, such as truck driving, may be associated with a risk of infertility. However, the research to support these links is mixed.
Risk factors
Risk factors linked to male infertility include:
- Smoking tobacco
- Using alcohol
- Using certain illicit drugs
- Being overweight
- Having certain past or present infections
- Being exposed to toxins
- Overheating the testicles
- Having experienced trauma to the testicles
- Having a prior vasectomy or major abdominal or pelvic surgery
- Having a history of undescended testicles
- Being born with a fertility disorder or having a blood relative with a fertility disorder
- Having certain medical conditions, including tumors and chronic illnesses, such as sickle cell disease
- Taking certain medications or undergoing medical treatments, such as surgery or radiation used for treating cancer